Analyst: Ioana Crisan, Human Services Research Institute, Director of Health Care Reporting
Director of Health Care Reporting
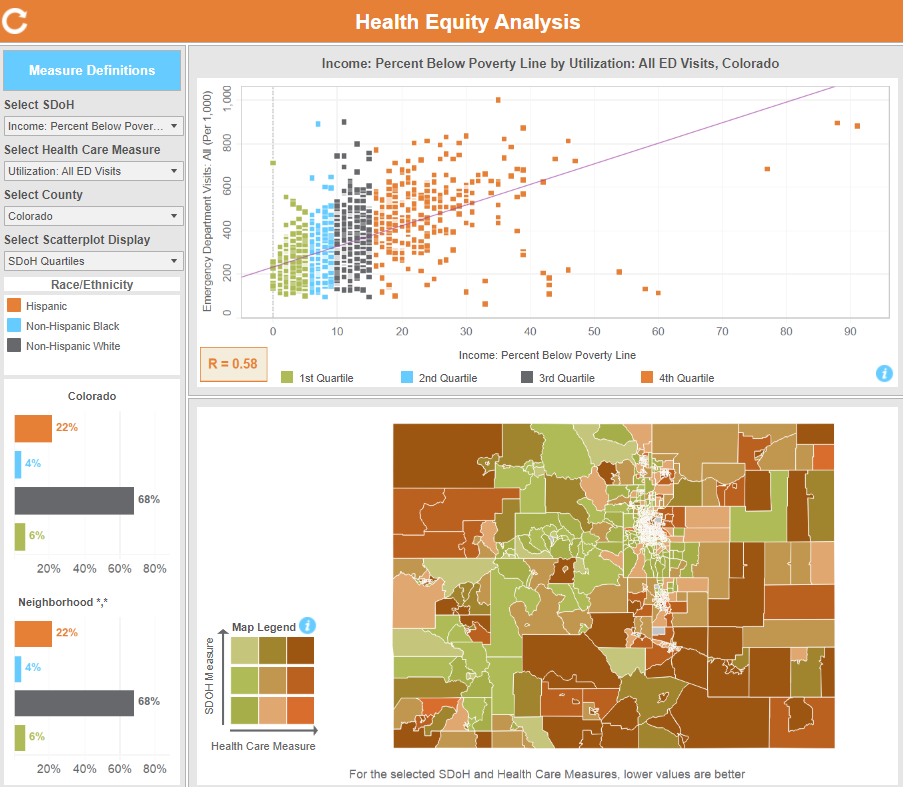
Project Name: Health Equity Analysis
Project Purpose: The Health Equity Analysis shows the relationship between key social factors and access, use, and cost of health care services that can impact a person’s health.
What were your first steps when beginning this analysis?
The idea to develop this type of analysis and visualization came from conversations with CIVHC’s former Director of Research and Performance Measurement, Maria de Jesus Diaz-Perez. We were discussing the importance of contextual information that speaks to the social and environmental conditions of neighborhoods where people live, and looking at how those factors impact health outcomes. We were aiming to develop a visualization that would support community organizations and other stakeholders to better understand the relationship between these sets of measures in Colorado. We had seen some good APCD-based analyses developed by other states and were excited creating an initial prototype. The version published on the CIVHC website has improved significantly from that initial version through the diligent work and thoughtful feedback from CIVHC and HSRI team members, as well as some of CIVHC’s external partners.